
Une bonne intention, une mauvaise théorie, un résultat aberrant Volume 2, issue 8, Octobre 2006, DOI: 10.1684/med.2006.0009
Concepts
With 11,172 deaths in metropolitan France in 2002, breast cancer is a major public health problem. It is responsible for 19% of women deaths from cancer and 31% of malignant tumor deaths before the age of 65. Mass screening has intensified in France over the past several decades. The size of the tumor has never ceased to decrease at the time of diagnosis, but the mortality rate has remained desperately stable from 1980 to 2000. Over the same period, the annual number of diagnosed breast cancer cases doubled. These findings bring into question the soundness of screening and the necessity to quantify overdiagnosis.
Bernard Duperray St Antoine Hospital, Radiology Department, Paris
Bernard Junod National School of Public Health, Assessment of risks related to the environment and the health care system Rennes
Keywords : benefit/risk, breast cancer, screening DOI: 10.1684/med.2006.0009
It is claimed that after an initial preclinical phase of several years, the threshold for clinical detection is reached when the tumor measures approximately 1 cm. Thanks to mammography, screening would take place 1 to 3 years earlier, thus limiting the possibility of developing metastases that would only occur at a given tumor size.
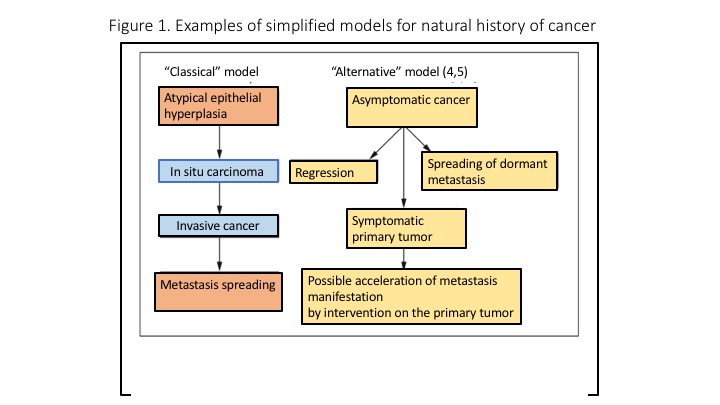
These phases are assumed to mechanically follow one another[1]. A small volume lesion would mean an early diagnosed lesion. “Small” and therefore “early” would be synonymous with curable. The classic pattern (Figure 1), where atypical epithelial hyperplasia develops into cancer in situ and then into invasive cancer which gradually increases to a critical size, suggests that the use of screening could be sufficient in breaking this sequence before invasive cancer develops.
Yet, clinical findings in daily practice show that the progression of the disease is neither linear nor obligatory over time. Sudden changes, static situations and even regressions are observed.”Small” does not mean “early”. A tumor can develop clinically in a few weeks or even days. A millimetre-sized lesion can be associated to metastases, just as a small tumor which can remain small for many years without becoming a deadly cancer. On the other hand, large, widespread tumors may have no radiological translation.
Although the size of the tumor is apparently associated with the prognosis, it is not with time. In his reference book on breast diseases[2], Professor Charles Gros noted as early as 1963: “The chances of survival with our locoregional therapeutics are linked to the small size of the intramammary lesions. But the smallness of intramammary lesions is only very partially related to time. There is no rigorous parallelism between early diagnosis in time and in space“. In most cases, ductal cancer in situ does not evolve into an invasive lesion .
A revision of more than 10,000 breast biopsies completed in Nashville, Tennessee, between 1952 and 1962, revealed cancers in situ in women who were considered not affected by cancer and therefore untreated. After 10 years, 75% of these women did not develop invasive cancer [3]. A wide range of potential clinical evolutions are observed for the same histological abnormality that defines breast cancer : some cancers develop and kill no matter what is done, others seem to respond to treatment, some remain silent, some regress or even disappear spontaneously. The alternative model diagram ( figure 1) takes into consideration these observations.
The question is to know whether these two types of cancer that can not be histologically distinguished are the same disease with varying evolutions, or whether they are entirely different entities with the same breast stigma.
At present, breast cancer in all its histological forms is a disease whose natural history is not well known and whose strictly histological definition is reductive at a given time, once associated with a linear evolutionary model.
The drop in mortality is not there in spite of screening
The only argument for continuing screening despite scientific evidence was the result of some randomized studies, such as the so-called “two Swedish counties” study published in 1985. It promised women who would be screened a 25-30 % reduction in breast cancer mortality.
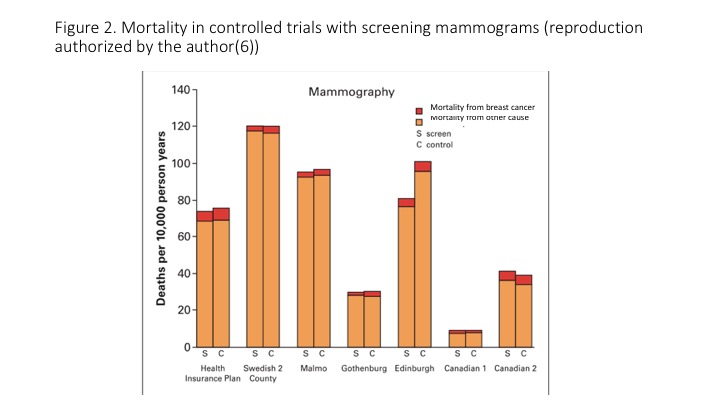
Examination of all the results of the seven controlled trials, including a mammography screening, shows the level of knowledge available on its effectiveness. Figure 2 illustrates, first of all, that the importance of mortality value varies between studies. This is mainly due to variations in the age structure of the cohorts of women studied. The greatest difference in mortality between the screened and the control group is noted in the Edinburgh and Guildford study. It is now acknowledged that this difference is the result of a flaw in the so-called random allocation of women to each group.
Thus, this study does not allow to argument for or against the screening.The second largest difference observed is headed in opposite direction in a Canadian study. This result also prompted to an expertise on the quality of random allocation.
However, after this expertise, the procedures used and the results obtained were considered as valid. Overall, the differences in mortality between studies are not coherent, both in terms of their meaning and their importance [6, 7]. This finding is consistent with the Cochrane review published in 2001 [8]. In particular, it highlighted the precarious nature of the study of the two Swedish counties and of the Health Insurance Plan in New York, once we take into account the method of drawing the samples, the comparability of the groups, the exclusions during the study after randomization and the way in which death was attributed to breast cancer. This may explain why in Sweden, where screening has the longest tradition, the gain in mortality noted in practice is insignificant: 0.8% for 11% expected.
Although the reduction in mortality is not met, the perverse effects are present
The title of the lecture presented in the summer of 1994 already by Dr. Marie-Hélène Dilhuydy asked the following question about screening : “A generous and life-saving purpose or a sanitary ideology with a perverse ethic, is the breast cancer screening useful for women ?” She clarified that mass screening probably reduces breast cancer mortality, but that the benefit is very limited and very difficult to demonstrate before alerting about the perverse effects that have already been observed. Since then, the extent of these effects has led to a continuous reconsideration of the practical modalities of screening.
False-positives
This refers to women who test positive even though they are not affected by cancer. The rate of false-positive mammograms has been particularly studied in Great Britain. Cumulative risk of false-positives after 10 mammography tests is 49.1%.
The positive predictive value (PPV) represents the probability that a woman with a positive test is affected by the disease. In France, the PPV for mammography testing using a single image per breast has never exceeded 9% at best, whereas a test judged as good should reach at least 30% or more [9]. Thus, 91% of women with a positive test were alarmed and had to undergo unnecessary diagnostic tests. The consequences are more and more aggressive complementary tests, including even biopsy, since it is becoming more and more difficult to reassure without histological evidence.
The evolution of the classification of radiological images according to the Breast Imaging Reporting and Data System (BIRADS) of the American College of Radiology (ACR) illustrates the difficulty of trying to make a practical attitude dependent on an imagery which is not very sensitive and not very specific.
The classification of microcalcifications in ACR 3, which should lead to easy monitoring, has been progressively diminished in favor of ACR 4, where histological verification is recommended. These tests are all the more inevitable as patients are firmly convinced that the smallest delay in diagnosis leads to a loss of chance and considerable prejudice [10].
Overdiagnosis and overtreatment
This is definitely a major deleterious effect of screening. It corresponds to diagnosis by excess. Overdiagnosis does not only concern cancers in situ but also invasive cancers that are slowly evolving or regressing spontaneously. It corresponds to the detection of cancer cells that would never have evolved.
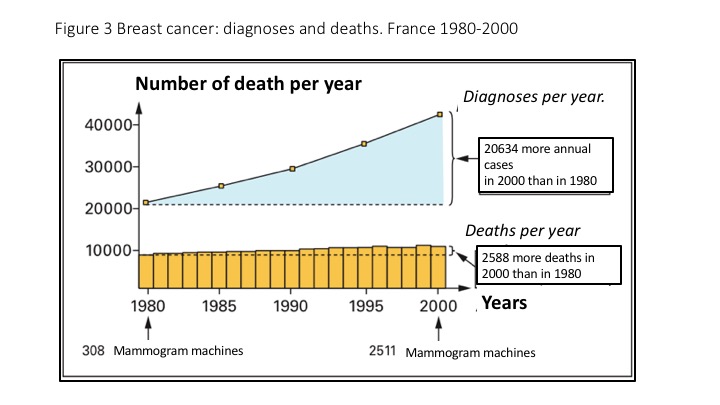
As shown in figure 3, there has been an “epidemic” increase in breast cancer diagnosis in France since 1980 [11]. How can that be explained?
An advance in diagnosis reaching an average of 12 months would only lead to 10% of the rise observed between 1980 and 2000. If this “epidemic” of diagnoses reflected a real increase in the incidence of progressive cancers, therapeutic effectiveness would have to be significantly improved. Indeed, we had only one cancer cured for a lethal cancer in 1980, while we have three cancers cured for a lethal cancer in 2000. In view of the results of controlled trials and the relative stability of treatment methods, such progress is implausible.
Another way to address the issue of over-diagnosis is to evaluate the reservoir of asymptomatic breast cancers present in the population of women. What is clinically observed is only the tip of the iceberg. Similarly to prostate cancer, there are occult breast cancers that will not reveal themselves during the patient’s lifetime. Evidence of this is illustrated by a series of autopsies performed on women who did not know they had breast cancer during their lifetime. Studies published between 1984 and 1988 provide the results of a systematic search for breast cancer in a series of autopsies that were not selected on the basis of breast pathology. They concern, for example, women who died of a violent death and were examined in a forensic medical institute.
The difference between the number of invasive cancers diagnosed at autopsy and the expected number estimated from the incidence data for the time is considerable: there are more invasive cancers and, above all, far more in situ cancers at autopsy. The discovery of these cancers was all the more frequent as the number of cuts made by anatomopathologists increased. Thus, the more we search, the more we find [12].
More recently, longitudinal observations have documented the existence of overdiagnosis. Since mammography screening has existed for several decades, there are now sufficient retrospective data to show that cohorts of women with multiple screening examinations in succession had significantly more diagnoses than those screened only at the end of an equivalent observation period [5, 13].
Overtreatment is a consequence of overdiagnosis, whose it enhances its deleterious effects. Paradoxically, the results of the treatment of quiescent or pseudo-cancers are always considered to be satisfactory since they do not threaten the woman’s life.
Importunate treatment
Several publications report the acceleration of metastases in vital organs following diagnostic and/or therapeutic interventions in breast cancer [4, 14]. Among the mentioned mechanisms, these authors suggest, for example, that a blunt diagnostic or therapeutic procedure releases circulating products responsible for stimulating metastases or that the excision of the primary tumor removes an inhibition of their growth.
Irradiations
Even if irradiation can be controlled and assessed by a quality procedure, its repetition in increasingly short periods of time represents an accumulation of small doses that increase the risk of cancer. According to estimates by the National Cancer Institute in the United States, an accumulated individual dose of 10 mSv would lead to between 9.9 and 32 cancers per million women. Patients carrying the BRCA genes show an increased radiation risk in vitro, yet they are proposed annual check-ups starting already at 30 years of age.
Perspectives of salutary advances?
Following the logic of a theoretical model based on the linear evolution of cancer, industrialized countries have engaged in screening programs to solve the problem of breast cancer mortality. The major concerns of French screening are currently of two kinds: its accessibility for all women and the improvement of senology practices. Thus, the National Cancer Institute is seeking to establish a culture of screening and to strengthen quality control, both in terms of the training of the practitioners involved and of the equipment they use. The interest in cancer screening has revealed its ineffectiveness. The indicators chosen to observe the disease do not allow progress to be made in understanding it. They create perceptions that contradict reality.
The mortality rate remains desperately stable in France, even though all the indicators used are reassuring: reduction in tumor size, reduction in the number of lymph node invasions and detectable metastases upon discovery of the disease, apparent improvement in survival at 5 or 10 years.
In most industrialized countries, two observed contradictory trends need to be clarified and quantified : on the one hand, iatrogenic effects due to inadequate therapies, considering the diversity of the evolution of the disease, of which the natural history is not well known, that contributes to deterioration of the prognosis, and on the other hand, therapeutic advancement in relation to better targeted treatments that improve survival.
In the current context, overdiagnosis inevitably leads to unnecessary and dangerous overtreatment, since lesions unjustifiably diagnosed as cancerous “diseases” would never have manifested themselves. Such “successes” are used to justify the continuation of the screening. They reassure practitioners that their activity is well-founded, while they only mask the ineffectiveness of the followed directions.
Potential improvements as a result of awareness-raising of the extent of the observed facts are considerable.
Conclusion
The willingness to act through systematic screening for a disease whose causes and natural history are not well known implies major disadvantages, in particular :
– unnecessary diagnostic tests;
– harmful treatment of tumors that would have had no consequences if they had not been diagnosed;
– possible acceleration of the manifestation of metastases;
– the induction of cancers by ionizing radiation in a healthy population.
A reorientation of research and health care is necessary to improve the specificity of the definition of cancer and limit the downside of a generalized systematic screening.
Conflicts of Interest: The authors declare that they have no conflict of interest in the subject covered by this article.
Summary: Breast Cancer Screening
Insufficiencies in the definition of breast cancer based on the results of punctual examinations and a linear theoretical model of the history of the disease bring into question the validity of its systematic screening.
Overdiagnosis and overtreatment are the major risks to avoid.
Click on images to enlarge
Références :
1. Ménégoz F, Chérié-Challine L, et al. Le cancer en France : Incidence et mortalité, situation en 1995 et évolution entre 1975 et 1995. Ministère de l’emploi et de la solidarité et réseau Francim eds. Paris : La Documentation française ; 1998.
2. Gros C. Les maladies du sein. Paris : Masson, 1963, 573 pp.
3. Page DL, Dupont WD, Rogers LW, et al. Continued local recurrence of carcinoma in situ 15-25 years after a diagnosis of low grade ductal carcinoma in situ of the breast treated only by biopsy. Cancer. 1995;76:1197-200.
4. Baum M, Demicheli R, et al. Does surgery unfavourably perturb the “natural history” of early breast cancer by accelerating the appearance of distant metastases? Eur J Cancer. 2005;41:508-15.
5. Zahl PH, Strand BH, Maehlen J. Incidence of breast cancer in Norway and Sweden during introduction of nationwide screening: prospective cohort study. BMJ. 2004;328:921-4.
6. Black CB, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst. 2002;94:167-73.
7. Mammographies et dépistage des cancers du sein. La revue Prescrire. 2006;272:348-71.
8. Olsen O, Gotzsche PC. Cochrane review on screening for breast cancer with mammo-graphy. Lancet. 2001;358:1340-2.
9. Renaud R, Gairard B, Schaffer P, Haehnel, Dale G. Définition et principes du dépistage du cancer du sein. 11 Journées de la Société Française de Sénologie et de Pathologie Mammaire, Tours, septembre 1989.
10. Berlin L. Malpractice issues in radiology. The missed breast cancer : perceptions and realities. AJR. 1999;173:1161-7.
11. Remontet L, Estève J, Bouvier et al. Cancer incidence and mortality in France over the period 1978-2000. Rev Epidemiol Santé Publique. 2003;51:3-30.
12. Welch HG. Dois-je me faire tester pour le cancer ? Peut-être pas et voici pourquoi. Laval ; Presses de l’université : 2005, 263 pp.
13. Zackrisson S, Andersson I, Janzon L et al. Rate of over-diagnosis of breast cancer 15 years after end of Malmö mammographic screening trial: follow-up study. BMJ. 2006;332:689-92.
14. Cox B. Variation in the effectiveness of breast screening by year of follow-up. J natl Cancer inst. Monogr 1997;22:69-72.
🛈 Nous sommes un collectif de professionnels de la santé, rassemblés en association. Nous agissons et fonctionnons sans publicité, sans conflit d’intérêt, sans subvention. Merci de soutenir notre action sur HelloAsso.
🛈 We are an French non-profit organization of health care professionals. We act our activity without advertising, conflict of interest, subsidies. Thank you to support our activity on HelloAsso.
